
If you have rheumatoid arthritis (RA), chances are you’ve wondered whether what you eat matters. You may have come across others with RA who swear that a certain diet has helped them, whether it’s a plant-based diet like the Paddison Programme or the Autoimmune protocol. You’ve heard some people avoid all animal foods and others embrace a meat only diet. It’s confusing.
My interest in the Paleo diet and its effect in rheumatoid arthritis began many years ago when I heard of several people with RA who used it, and experienced a large reduction in their symptoms.
This led to my desire to test the AIP diet in a clinical study. In 2021 I began this research as the first part of my PhD. Despite the AIP diet being popular, until this study, it had never been tested in any type of clinical trial.
Initial studies are often structured as a pilot study, designed test the feasibility, time, cost, and adverse events of the planned research methods.
What Is the AIP Diet?
The Autoimmune Protocol is an intensive elimination-and-reintroduction diet, originally developed by Professor Loren Cordain and later expanded by biophysicist Sarah Ballantyne. It starts from a paleo framework and goes considerably further. Up to date information on the AIP diet and lifestyle is now on the Autoimmune Wellness website.
The AIP diet used in the study is the core AIP version which is the most restrictive.
The elimination phase excludes: grains, pseudograins, legumes, dairy, eggs, nightshade vegetables (tomatoes, capsicum, chilli, potatoes, eggplant), nuts and seeds, alcohol, sugar, seed oils, and all food additives – including synthetic colours, flavours, emulsifiers, and preservatives.
Foods allowed are: unprocessed meats, poultry and seafood, all fruits and vegetables (except nightshades), fermented foods, organ meats, olive oil, coconut oil, avocado, and alternative flours that come from vegetables or fruit- like cassava, green banana, tigernut, and coconut. Herbs and spices from leaves, bark, flowers or pods are allowed.
The rationale is biological: these excluded foods may increase intestinal permeability, potentially allowing dietary and microbial antigens to enter systemic circulation and drive autoimmune activity. In RA, which is characterised by gut microbiome disruption and increased intestinal permeability, this is plausible although it isn’t proven that all these foods have this effect.
Study Design
Nine adults with a confirmed RA diagnosis from Auckland, New Zealand participated in this 12-week pilot study. The design was a single-arm crossover:
- Weeks 1–4: Participants continued their usual diet (control phase)
- Weeks 5–12: Participants followed the AIP elimination diet
No food was provided. Participants shopped and cooked for themselves, received a detailed instruction booklet and a one-hour session with Julianne – a Registered Nutritionist, and had access to ongoing support via a private Facebook group and direct researcher contact.
We measured two validated patient-reported outcome (PRO) tools weekly:
- RAPID3 (Routine Assessment of Patient Index Data 3): assesses RA disease activity on a 0–10 scale; correlates with clinician-assessed disease activity scores like DAS28-CRP
- RAID (RA Impact of Disease): captures seven domains most important to patients – pain, physical function, fatigue, sleep, physical wellbeing, emotional wellbeing, and coping
We also collected three-day weighed food records, weight and waist circumference measurements, and weekly adherence checklists.
What Happened: The Results
Disease Activity (RAPID3)
At the start of the intervention, participants’ mean RAPID3 score was 2.73/10. By week 12, it had dropped to 0.99/10 – below the threshold for remission (≤1.0).
Looking at individual responses (which is more meaningful in a small study than group averages):
- 4 participants achieved a “good” RAPID3 response — a reduction of more than 1.2 points reaching an endpoint below 2.0
- 3 participants moved into remission from low disease activity
- 1 participant’s scores worsened during the intervention
- The most notable improvements appeared between weeks 6 and 8 of the AIP phase
This graph shows the trajectory of each person’s RAPID3 results (participant numbers 8 and 9 withdrew before the AIP diet phase) :

RA Impact (RAID)
Mean RAID scores dropped from 3.13/10 to 1.02/10. Seven of nine participants improved.
- Three participants reduced their RAID score by more than 3 absolute points
- By week 8, seven of nine participants had RAID scores below 1.5 — indicating a “patient-acceptable symptom state”

Fatigue and Sleep: Surprisingly Strong Reductions in Scores
The results that excited me to see, were the changes in fatigue and sleep scores. These are two domains that people don’t experience a lot of improvement in, despite modern RA medications.
Mean fatigue scores dropped from 4.44/10 to 1.11/10 by week 12. Eight of nine participants finished with a score of 0 or 1. One participant who also had fibromyalgia reported a fatigue score dropping from 10 to 1.
Sleep scores also improved, from a mean of 3.77/10 to 1.22/10.
Pain Medication Use
Mean weekly NSAID (anti-inflammatory) use fell from 1.97 doses per week during the habitual diet phase to 0.11 doses per week at the end of the AIP intervention. Paracetamol (pain relief) stayed about the same.
Weight and Body Composition
Weight loss wasn’t an intended outcome, but eight of nine participants lost weight during the AIP phase, with a mean reduction of 5 kg. Mean BMI decreased from 26.3 to 24.5 kg/m², and mean waist circumference reduced by 4.8 cm. Participants consistently reported greater satiety on the AIP diet despite eating freely to appetite.

What Changed in Their Diets?
There were some quite large dietary shifts. Compared to their habitual diets, participants on AIP:
- Increased vegetable intake from a median of 4.5 to 11.5 servings per day
- More than doubled fruit intake
- Tripled seafood consumption
- Increased daily fibre from 25.5g to 35.6g
- Dropped refined grain intake from ~5 servings per day to zero
- Reduced added sugar from 31g to 17g per day
- Eliminated alcohol entirely
This resulted in increased long chain omega 3, potassium and vitamin C. However two nutrients declined considerably – calcium (due to dairy exclusion) and iodine (due to lower salt intake and exclusion of dairy, eggs, and commercial bread)
Adverse Effects in Two People
While seven people experienced improvements, two had some persistent adverse effects: one developed regular diarrhoea from week five (likely related to a very substantial increase in fibre and fruit intake), and another reported persistent lethargy, loss of appetite, and unintended weight loss, along with increased RA symptoms. The cause is unknown, and may be a worsening of symptoms that may have happened regardless, or addition of new foods like cassava (some people have reported cassava causing autoimmune flares)
Cost and Ease of Implementation
Participants generally reported higher food expenses at the beginning of the intervention, primarily due to the need to purchase AIP-compliant pantry staples. However, some participants who frequently dined out reported reduced overall spending. The first 3-4 weeks there was a high mental load putting the new diet into practice, however it became easier after this. Cost and implementation compared to habitual diet.

What is Next?
The AIP diet is very restrictive, and as well as excluding foods, diet quality increased, leaving us to wonder to what extent quality affected the results, whether all these food exclusions are necessary. If the clinical benefit can be achieved with fewer restrictions, that’s critical information for clinicians and patients alike.
We are planning another study which we hope will partially answer this question.
You can find the full published study here:
What the Study Doesn’t Tell Us
This was a feasibility pilot – nine people, no control group, and a complex dietary intervention.
Some important caveats:
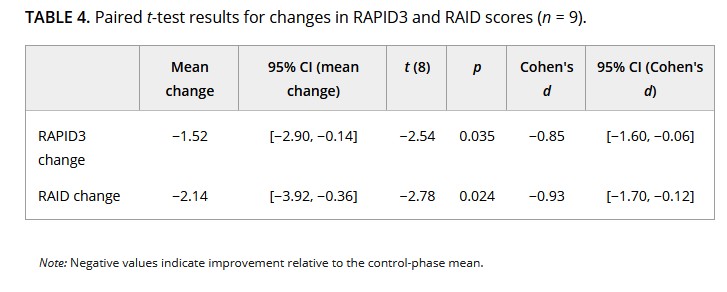
Small sample size. Nine participants is not enough to draw definitive conclusions. Individual variation was high, and one participant clearly worsened. (However the Cohen’s d tells us result was a large effect)
No control group. We can’t rule out that improvements were due to the passage of time, increased attention, or other lifestyle changes that occurred alongside the dietary shift.
Participant selection. People who volunteer for an intensive dietary study are likely highly motivated – and this showed in their adherence. Results may not translate to a broader RA population.
Low baseline disease activity. About half the participants had low disease activity at baseline, which limits our ability to detect the full potential of the intervention. A future trial needs to recruit people with moderate-to-high disease activity to give the treatment a real chance to demonstrate meaningful change.
COVID-19 lockdown. The study ran during New Zealand’s 2021 lockdown, which likely affected adherence patterns (for better and worse – social eating situations are a major challenge for elimination diets).
No inflammatory biomarkers. We measured how people felt, not what their inflammatory markers were doing. A future study needs objective measures like CRP, ESR, and ideally gut health biomarkers.